Pityriasis rubra pilaris (PRP) is a rare, chronic inflammatory skin disorder characterized by distinctive reddish-orange scaling patches, rough bumps centered around hair follicles, and a waxy thickening of the palms and soles [cite: 3973, 3974, 4019]. PRP exists as a diverse disease spectrum that can vary from localized patches in children to widespread redness covering the majority of the body in adults [cite: 3977, 3980, 4019]. While managing this complex condition can be challenging, a professional skin biopsy, modern targeted biological therapies, and collaborative healthcare support can successfully clear the skin and restore your quality of life [cite: 3996, 4005, 4011, 4024].
What Is Causing This Reddish-Orange Scaling Rash?
Understanding how your body’s immune system signaling interacts with skin cell development is a strategic first step in managing PRP. The exact primary cause of most cases of PRP remains unknown (idiopathic) [cite: 3985]. However, modern medical research has revealed that the condition is driven by a deep structural overactivation of the Th17/IL23 inflammatory pathway [cite: 3987]. This is the exact same biological signaling network implicated in psoriasis [cite: 3987]. When this immune highway is triggered, it accelerates skin cell proliferation and disrupts normal cell maturation [cite: 4059].



You can think of a PRP flare-up as an “immune system runaway train.” This internal biological response prompts your skin cells to produce excessive keratin, leading to follicular plugging and rough scaling [cite: 3974, 4038]. Identifying this condition early via clinicopathological correlation is the essential “So What?” factor in your recovery plan [cite: 4022]. Because it involves distinct cellular pathways, traditional treatments like standard topical steroids are often completely insufficient, making it necessary to implement advanced, pathway-targeted systemic regimens [cite: 4006, 4008, 4022].
Understanding the Visual Profile: The Hallmarks of PRP
PRP presents with highly specific clinical features that change as the condition moves across the skin. Recognizing these architectural landmarks prevents medical confusion and assists your provider in confirming an accurate diagnosis [cite: 3995].
| Clinical Sign | Visual Appearance and Anatomic Behaviors |
|---|---|
| Follicular Papules | Small, pointed, reddish bumps centered strictly around hair follicles [cite: 3974, 4038]. They feel rough and coarse, creating a distinct “sandpaper-like” or nutmeg-grater texture upon physical palpation [cite: 3974, 4076]. They are most prominent on the dorsal fingers, elbows, and knees [cite: 3982, 4076]. |
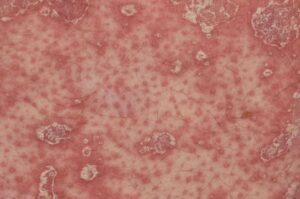
| Islands of Sparing | Highly characteristic, small round patches of completely normal, unaffected skin left untouched right in the middle of vast fields of bright red-orange inflammation [cite: 3976, 4075]. This is an invaluable diagnostic milestone for your provider [cite: 3995, 4075]. |
| Palmoplantar Keratoderma | A profound, uniform thickening of the skin on the palms of the hands and soles of the feet [cite: 3975, 4058]. This tissue takes on a highly unique, smooth, waxy, and yellow-orange color profile that is prone to developing deep, painful cracks (fissures) [cite: 3975, 4076]. |
| Erythroderma | An advanced stage where intense redness and sheets of fine, flaky scale expand to cover virtually the entire body surface [cite: 3977, 4037]. This severe manifestation disrupts your body’s temperature regulation, mimicking a total skin burn [cite: 3977]. |
Am I at risk for Pityriasis Rubra Pilaris?
Developing PRP is an isolated, unpredictable biological event. It has absolutely zero connection to personal cleanliness, hygiene flaws, or dietary mistakes.
- The Age Axis: PRP can affect individuals of all ages [cite: 4015, 4016]. It exhibits a bimodal onset, peaking in childhood and adolescence as **juvenile-onset PRP**, and rising again in adults over the age of 50 as **classical adult-onset PRP** [cite: 3981, 3982].
- Genetic Mutations: Inherited or familial forms of PRP, which typically surface very early in childhood, are directly associated with genetic mutations in the **CARD14 gene** [cite: 3986, 3990].
- Medication Triggers: Developing a sudden PRP-like eruption has been linked to the use of targeted oncological therapies, specifically **kinase inhibitors** (such as ponatinib) [cite: 3988, 3991, 4062].
- Systemic Viral Status: One specialized, severe subtype of the condition is directly associated with underlying **HIV/AIDS** immune alterations, making viral screening an important baseline step [cite: 3993].
Where and How It Appears on My Body
PRP leaves a very specific anatomical “map” as it progresses across the skin layers, guiding your clinical team toward an accurate diagnosis [cite: 3995].
- The Cephalic Cascade: In the classic adult form, the condition begins as an intense, dry scaling on the scalp, face, and neck, mimicking severe seborrheic dermatitis before expanding down the torso [cite: 3981, 4001].
- The “Waxy Sandal” Soles: Thickening focuses heavily on the palms and soles, creating a hard, leather-like yellow layer that can envelop the entire bottom of the foot [cite: 3975, 4076].
- Leonine Facies: In erythroderma, extensive cellular infiltration into the facial tissue can cause permanent skin thickening and heavy skin fold wrinkling, giving the face a coarse, lion-like appearance.
- Nail Architecture Changes: The disease frequently targets the nails, causing severe thickening of the nail plate, yellow-brown discoloration, subungual debris, and tiny vertical lines of bleeding under the nail known as **splinter hemorrhages** [cite: 3978, 4067].
Solutions I Can Try at Home
Because moderate-to-severe PRP is a systemic, internally driven inflammatory process, at-home measures focus entirely on skin lubrication, comfort support, and protecting the fragile skin barrier [cite: 4006, 4021].
- Aggressive Emollient Lubrication: This is the single most vital at-home tool [cite: 4006]. Apply thick, fragrance-free emollient creams or plain white petrolatum ointments multiple times a day to trap moisture, soften rough scales, and ease the tight, pulling sensation of erythrodermic skin [cite: 4006, 4035].
- Keratolytic Foot Care: For waxy, thickened skin on the palms and soles, use over-the-counter creams containing high concentrations of **urea or salicylic acid** to safely dissolve the hard keratin bridges and reduce painful cracking [cite: 4007, 4051].
- Enforce a Cool Environment: Avoid hot showers, saunas, and strenuous exercise that causes heavy sweating. Staying in cool climates directly quiets active skin-directed nerve endings and minimizes severe itching flares [cite: 3678].
- Mental Health and Community Tracking: Because PRP changes your appearance dramatically, it can cause severe emotional distress [cite: 4023]. Actively engage with established support networks like the **PRP Alliance** to protect your mental well-being [cite: 4025].
When Should I See a Dermatology Provider?
PRP is a complex, progressive condition that requires expert dermatological oversight. Because its early stages look identical to common psoriasis or severe eczema, your provider must perform a safe, in-office **4mm punch skin biopsy** to evaluate the cellular architecture and exclude more serious lookalikes [cite: 3996, 3998].
Seek Professional Help if You Notice These Warning Signs:
- Rapidly Spreading Erythroderma: Your red-orange scaly patches begin spreading rapidly to cover the majority of your body surface, indicating a progression toward erythroderma that requires immediate systemic triage [cite: 3973, 3977, 4037].
- Impaired Range of Motion: The yellow keratoderma on your palms or soles grows so thick, tight, and cracked that it prevents you from closing your hands, gripping objects, or walking comfortably on your feet [cite: 3975, 4019, 4058].
- Diagnostic Uncertainty: You are experiencing an aggressive, rough, sandpaper-like rash that has completely failed to improve with standard over-the-counter hydrocortisone or low-potency steroid creams [cite: 3974, 4006, 4076].
- Organ Signaling Concerns: Long-standing systemic skin changes are accompanied by severe eyelid turning outward (**ectropion**), shivering, chills, or widespread lymph node swelling, indicating a breakdown in your skin’s regulatory safety [cite: 4033, 4054].
Frequently Asked Questions
- Q: Why are modern biological therapies preferred over traditional medications for PRP?
A: Historically, providers relied on traditional systemic treatments like oral methotrexate or acitretin [cite: 4010]. However, modern dermatological clinical trials have shown that newer **biologic medications targeting the IL-17 or IL-23 pathways** (such as ixekizumab, secukinumab, or risankizumab) demonstrate significantly higher efficacy rates and provide rapid, deep skin clearance by blocking the exact immune highway driving the disease [cite: 3987, 4011, 4022]. - Q: What important lab monitoring is required if I am prescribed oral Isotretinoin?
A: Oral isotretinoin or high-dose retinoid therapies can be highly effective for moderate PRP [cite: 4009, 4048]. However, because these medications are processed heavily through the liver and influence systemic fat profiles, you must undergo regular blood tests. Your provider will execute baseline and routine laboratory monitoring of your **liver function tests (LFTs) and fasting lipid levels** (triglycerides) to ensure complete safety throughout your treatment course. - Q: What is the long-term prognosis of PRP, and will it return after it clears?
A: The long-term outlook varies significantly based on when the condition surfaced. Approximately 50% of classical adult-onset cases undergo completely **spontaneous resolution within three years**, and once cleared, a permanent recurrence is exceptionally rare [cite: 4015, 4017]. Conversely, childhood or juvenile-onset cases are statistically more likely to follow a chronic, lifelong course that requires ongoing long-term medical maintenance [cite: 4016].
The long-term outlook for adult-onset pityriasis rubra pilaris is highly encouraging, as the underlying immune flare is pre-programmed to resolve or stabilize over time under proper guidance [cite: 4015]. Success relies on early clinicopathological verification, strict adherence to barrier lubrication, and close partnership with a multidisciplinary clinical team to navigate your recovery smoothly [cite: 3996, 4006, 4024].