Quick Summary: Melanoma is a potentially serious form of skin cancer that originates within the pigment-producing cells of the skin, known as melanocytes [cite: 1850, 2050]. It can manifest on any skin surface, as well as on mucous membranes or the eyes [cite: 1897, 2040]. Because early detection is the single most important factor for an excellent prognosis, regular self-skin evaluations and prompt clinicopathological verification via a professional skin biopsy are critical milestones to eliminate the tumor and protect your long-term health [cite: 1927, 1956, 1960, 2035, 2042, 2044].





What Is Causing This Type of Skin Cancer?
Understanding how cellular changes and environmental stressors interact within your skin layer is a strategic first step in managing your health tracking. Melanoma develops when the pre-programmed genetic code within your melanocytes suffers severe damage, transforming normal cells into an atypical, rapidly multiplying population [cite: 1850, 1905, 2050]. This condition is entirely independent of personal lifestyle errors, hygiene flaws, or basic skin allergies.
The primary environmental driver of almost all cutaneous melanomas is exposure to ultraviolet (UV) irradiation from natural sunlight or artificial tanning beds [cite: 1905, 1911, 2056]. This radiation causes critical genetic breaks and triggers specific mutations in somatic pathways—such as CDKN2A gene lines—disrupting your cells’ natural tumor-suppression and DNA-repair mechanisms [cite: 1906, 1909, 1921].
As these atypical cells continue to divide, they typically undergo a slow, horizontal spread restricted completely to the outer skin layer, known to clinicians as the radial growth phase [cite: 1860, 2057]. If left unmanaged, however, the cells can shift into a rapid, vertically oriented growth phase, physically breaking down the basement membrane to invade the deeper dermal layers and gain access to circulatory channels [cite: 1860, 2058, 2059]. You can think of a melanoma as an active “cellular processing failure” prompted by cumulative radiation stress [cite: 1905, 1906]. Identifying these changes early through a professional examination is the absolute “So What?” factor in your care plan [cite: 1925, 2042]. Catching a lesion during its earliest radial phase simplifies surgical removal and delivers an outstanding long-term cure rate [cite: 1860, 1956, 1960].
Understanding Your Skin Status: Tracking the Four Clinical Subtypes
Melanoma does not present as a uniform spot; instead, it encompasses four major physical variants that follow distinct visual timelines and geographical layouts across your body [cite: 1853, 1897]. Recognizing these structural behaviors prevents clinical confusion and ensures your care team applies the appropriate diagnostic approach [cite: 1925, 2081].
| Melanoma Subtype | Key Differentiators, Demographics, and Visual Layouts |
|---|---|
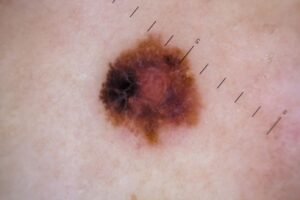
Superficial Spreading Melanoma (Most Common Form) | Features: Accounts for approximately 70% of all cutaneous cases, classically diagnosed between 30 and 50 years of age [cite: 1868, 1869]. It surfaces as an asymptomatic flat patch or slightly raised plaque with jagged, notched borders and varied, multicolored shades of tan, brown, and black [cite: 1866]. Anatomy: Demonstrates a strong biological preference for the lower legs in females and the upper trunk in males [cite: 1898]. |
| Lentigo Maligna Melanoma | Features: Most frequently diagnosed in the seventh decade of life, demonstrating a slow, horizontal growth phase that extends over many years [cite: 1863, 1864]. It presents as a large, asymmetric, flat brown-to-black macule with irregular, indented borders and variegated, mottled coloring [cite: 1862, 1865]. Anatomy: Maps its profile strictly onto chronically sun-damaged landscapes, clustering on the face, nose, and cheeks [cite: 1862, 1900]. |
| Acral Lentiginous Melanoma | Features: Represents the most common melanoma subtype found in patients with darker skin types, accounting for up to 70% of diagnoses in dark-complected persons and 45% in Asian populations [cite: 1871, 1872]. It forms asymmetric macules with irregular edges and prominent pigment variation [cite: 1870]. Anatomy: Restricts its visual layout to the hairless skin covering the palms of the hands, the soles of the feet, and the areas beneath the nails (subungual tissue) [cite: 1870, 1901]. |
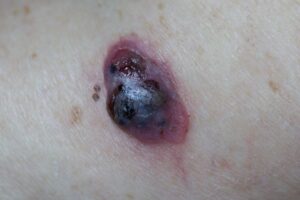
| Nodular Melanoma | Features: An aggressive, rapidly growing variant that bypasses a long horizontal phase, presenting directly as a firm, raised blue, black, red, or skin-colored nodule [cite: 1883]. It is statistically more common in men and has a high tendency to bleed, crust, or ulcerate [cite: 1883, 1884]. Anatomy: Frequently populates the trunk, head, and lateral neck regions [cite: 1899]. |
Am I at risk for Melanoma or systemic spread?
Developing melanoma is an interactive medical event driven by inherited genetic architecture and cumulative environmental triggers [cite: 1905, 2041]. Anyone can contract this condition, but specific profiles significantly elevate your long-term clinical risks [cite: 1908, 2047].
- The High-Risk Phenotype: Individuals possessing fair skin, red or blonde hair, freckles, and an unacclimatized skin barrier that burns easily before tanning carry a documented susceptibility to UV-induced Breaks [cite: 1913, 1923]. A personal history of frequent, blistering sunburns during childhood is a massive primary multiplier [cite: 1912].
- The Mole and Nevus Count Matrix: Having a high volume of spots alters your screening requirements [cite: 1914]. Susceptibility multiplies exponentially if you possess more than 50 standard moles (melanocytic nevi) larger than 5mm, have more than 5 atypical moles, or carry a verified family history of atypical/dysplastic nevus syndrome [cite: 1914, 1915, 1916].
- The Subungual Hutchinson Sign: When acral melanoma settles inside the nail matrix, it classically forms a longitudinal brown or black band across the nail plate [cite: 1875, 1949]. A critical warning indicator occurs if this linear pigment actively bleeds or extends upward onto the surrounding skin of the proximal or lateral nail fold—a clinical footprint known as a **Hutchinson sign** [cite: 1875, 1880, 2078]. New linear nail lines arising between 40 and 60 years of age, or any band wider than 3mm, require prompt evaluation [cite: 1881].
- The Immune Phenomenon of Regression: Up to two-thirds of melanoma cases display areas of spontaneous clearing, seen visually as white, faded, or lightened patches inside a dark mole [cite: 1854, 1895]. This is known as regression; rather than indicating the spot is healing, it reflects an intense interaction where your immune system is actively battling a progressing tumor, requiring close specialized tracking [cite: 1895, 1906].
Where and How to Scan Your Skin: The ABCDE and Ugly Duckling Framework
Melanoma can populate any anatomical corridor—including sun-protected spaces, mucosal zones (mouth, larynx, vagina, anus), and the chambers of the eye—making systematic visual mapping essential [cite: 1892, 1897, 1902, 1903, 2040].
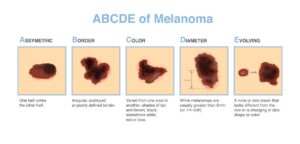
To safely track changes, you must utilize the gold-standard ABCDE assessment template during your monthly exams [cite: 1857, 2043]:
- A – Asymmetry: Drawing a clean line directly down the center of the spot reveals that one half does not match the structural layout of the other half [cite: 1857].
- B – Border Irregularity: The outer edges or margins of the patch are poorly defined, scalloped, notched, or jagged, rather than a smooth, neat circle [cite: 1857, 1866].
- C – Color Variation: The color is mottled and uneven, displaying a shifting mixture of dark brown, black, pink, or gray tones within a single lesion [cite: 1854, 1857].
- D – Diameter Expansion: The spot measures larger than 6.0mm (approximately the size of a standard pencil eraser), though smaller melanomas are regularly captured [cite: 1857].
- E – Evolution and Enlargement: This represents your **single most critical warning signal** [cite: 1858]. Any mole or skin lesion that undergoes a history of documented change in size, shape, thickness, or color, or begins itching, aching, or bleeding unprompted, requires immediate evaluation [cite: 1858, 1925].
The “Ugly Duckling” Sign: Always look for the outlier [cite: 1858]. If a pigmented spot appears noticeably darker, lighter, larger, or architecturally different from all the surrounding common moles on your body, it meets the criteria for the **ugly duckling sign** and warrants an immediate clinical checkup [cite: 1858].
Solutions I Can Try at Home
Because melanoma is an active, invasive skin malignancy driven by deep somatic gene breaks, over-the-counter anti-itch lotions or home remedies provide zero benefit and can cause dangerous medical delays [cite: 1905, 1927, 2066]. At-home care focuses entirely on mechanical shielding and strict protective surveillance [cite: 1956].
- Perform Meticulous Monthly Self-Exams: Establish a fixed monthly routine to examine your skin surface [cite: 1956, 2042]. Utilizing a full-length mirror and a hand-held mirror under bright, direct light, systematically map your skin [cite: 1926]. Be sure to inspect hidden corridors including your scalp, behind your ears, your nail plates, the soles of your feet, and your back [cite: 1901, 1926].
- Implement Strict Daily Photoprotection: Apply a broad-spectrum physical sunscreen daily to all exposed areas, wear wide-brimmed hats, and protect your limbs with tightly woven sun-clothing [cite: 2047]. Cutting off UV exposure protects your cellular pathways and shields surrounding sun-damaged landscapes [cite: 1911, 2056].
- Never Vigorously Scrub or Scratch a Spot: If you identify a changing mole or a crusted, bleeding nodule, leave it completely alone [cite: 1858, 1883]. Do not pick at the tissue or try to scratch the crust away; manual irritation will only cause localized bleeding and painful inflammation without removing the tumor cells [cite: 1883, 1927].
When Should I See a Dermatology Provider?
Melanoma can hide or mask itself as a benign seborrheic keratosis, a common blood blister under the nail, or a pigmented basal cell carcinoma [cite: 1951, 1952, 1953]. Seeking professional clinical triage early ensures you secure an accurate diagnosis via an expert pathology report [cite: 1927, 2044].
Consult Our Office Immediately if You Notice These Warning Signs:
- A Mole Meeting any ABCDE Criteria: You identify an old or new spot that displays expanding asymmetry, jagged borders, multicolored texturing, or measures larger than 6mm [cite: 1857].
- A Rapidly Growing, Firm Nodule: A new blue, black, or reddish bump emerges on your limbs, head, or neck and enlarges rapidly over a matter of weeks [cite: 1883, 1899].
- Persistent Nail Plate Pigmentation: You observe a dark linear band tracking down your nail bed that widens over time, features variegated streaks, or displays a visible Hutchinson sign on the surrounding cuticle skin [cite: 1875, 1880, 1882].
- An Evolving “Ugly Duckling” Outlier: A skin spot begins to shift in size, bleeds easily without being scratched, or looks completely different from every other mole on your body [cite: 1858].
Frequently Asked Questions
- Q: What primary in-office surgical biopsy and removal protocols are executed for early melanoma?
A: If a clinical suspicion is triggered, your provider will perform a definitive diagnostic intervention [cite: 1927]. Best practice requires executing a **complete full excisional biopsy of the entire lesion** with narrow safety margins rather than slicing across it [cite: 1928]. If a full excision is anatomically unfeasible, your provider will perform multiple, targeted 4mm punch biopsies specifically selecting the darkest or most variegated areas of the tumor to capture the deep tissue layout [cite: 1929, 1930]. If the pathology report confirms a **Melanoma In Situ (Stage 0)**, your dermatologist will cleanly remove the tumor via a formal wide local excision utilizing clear **7–10 mm surgical margins**, or complete an in-office Mohs Micrographic Surgery procedure to achieve a total cure [cite: 1961, 1990]. For early, thin **Invasive Melanoma less than 0.7mm in depth** with few visible cell divisions (mitoses), your provider will execute a wide excision utilizing a **10mm (1 cm) surgical margin** [cite: 1963]. - Q: When is a Sentinel Lymph Node Biopsy (SLNB) required, and how does it protect my health?
A: If your diagnostic biopsy reveals an invasive tumor **greater than 0.7mm in depth**, or a thin melanoma displaying a high volume of active mitoses, your provider will initiate a high-risk safety protocol [cite: 1931, 1964, 1965]. They will refer you directly to a specialized surgical oncologist for a wide local excision combined with a **Sentinel Lymph Node Biopsy (SLNB)** [cite: 1931, 1965]. This less traumatic procedure utilizes intraoperative lymphatic mapping to identify and remove the single, primary “sentinel node” that serves as the direct draining basin for the tumor site [cite: 1979, 1980, 1981]. Executing an SLNB delivers vital information on subclinical, microscopic lymph node status (micrometastasis) with minimal physical morbidity, helping to guide early therapeutic node dissections or identify candidates who will benefit from advanced systemic adjuvant treatments [cite: 1976, 1978, 1983, 1984, 1985]. - Q: What advanced staging guidelines and long-term surveillance checkup schedules are mandatory?
A: Your definitive staging is calculated directly from your histopathologic report by measuring your precise tumor thickness—known as **Breslow depth**—calculated from the top of your epidermis’s granular layer down to the deepest point of cell invasion, while factoring in surface ulceration and node status [cite: 1988, 2036, 2046]. If you are diagnosed with a thick tumor **greater than 2.0mm featuring surface ulceration (Stage IIB or IIC)**, your team will immediately order advanced whole-body **PET scans, chest/abdominal CT scans, and a brain MRI** to check for hidden internal disease, referring you to a medical oncologist for advanced immune checkpoint therapies (PD-1 inhibitors) or targeted BRAF-MEK inhibitors [cite: 2012, 2029, 2031]. To ensure absolute lifelong safety, patients must adhere to a strict surveillance schedule: returning for thorough professional full-body skin examinations and manual lymph node palpation **every 3 months for the first 2 years, weaning to every 6 months for the next 3 years, and continuing meticulous annual skin checks for life** [cite: 1957, 1806].
The long-term outlook for individuals managing melanoma is outstanding when the condition is detected and treated early in its development, as tumor thickness remains the single most powerful prognostic indicator for survival [cite: 1960, 2035, 2036, 2046]. Success relies on maintaining strict monthly self-examination habits, practicing daily broad-spectrum photoprotection, and strictly adhering to your multi-year clinical surveillance follow-ups with your interprofessional care team to keep your body safe, healthy, and fully protected [cite: 1956, 1957, 2042, 2047].